
Rotator Cuff Tears
By Dr. Bruce Blackstone M.D.
What is the rotator cuff?
The rotator cuff is a group of small muscles originating on the shoulder blade (scapula) and joining together to form a tendon that inserts on the upper arm (humerus) and thereby surrounds the ball and socket (shoulder) joint.
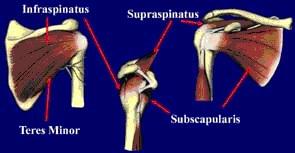
The function of the rotator cuff is twofold: It helps rotate the arm on its long axis (internal and external rotation) and more importantly, it functions to center the humeral head in the socket. The large muscles of the shoulder girdle (deltoid, latissimus, pectoralis major) as they function tend to displace the humeral head from the socket. A properly functioning rotator cuff prevents this displacement, whereas a torn or weak tendon cannot perform this centering function and pain and disability may result from this abnormal motion.

Normal rotator cuff and biceps
How does one injure the rotator cuff?
The rotator cuff may be torn as a result of a significant discrete trauma such as a fall, jerking or pulling force or a dislocation. More commonly, it can occur gradually with an insidious onset of pain and weakness due to repetitive microtrauma from overhead work or throwing activities, and also attritional changes in the tendon associated with aging and inherently poor blood supply to the tendon.
My shoulder hurts. Have I injured my rotator cuff?
Rotator cuff injuries are one of the most common shoulder problems in throwing athletes and also in the general population age 40 and over. Pain, however, is a nonspecific symptom of many different problems involving the shoulder, which underscores the importance of a comprehensive evaluation by a physician thoroughly familiar with the shoulder, such as an orthopedic surgeon.

Torn biceps tendon
Osteoarthritis (DJD) of shoulder
Pain is frequently described as aching in quality and is often felt on the side of the upper arm. It is often worse at night. The pain can also be "sharp and catching" with certain motions. The pain from rotator cuff injuries frequently co-exists with other conditions and must be distinguished from them. These may include acromioclavicular or glenohumeral (shoulder joint) arthritis, biceps lesions, labral tears, instability and adhesive capsulitis.

Labral tear
Weakness is also a common complaint and can be due to actual mechanical dysfunction associated with a large tear in the cuff or can be secondary to pain from an inflamed or partially torn tendon. Neurologic conditions such as cervical nerve root impingement or axillary or suprascapular nerve lesions may also manifest themselves as weakness and/or pain in the shoulder.

Severe weakness and inability to actively raise the arm to the side can result from a large tear in the rotator cuff and must be distinguished from passive restrictions of motion due to conditions such as glenohumeral arthritis and adhesive capsulitis.
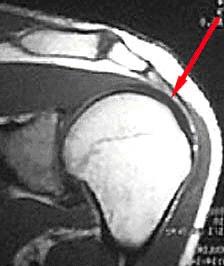
In addition to the types of symptoms experienced by the patient and the physical exam findings, imaging studies are often very useful in diagnosing rotator cuff injuries. Plain radiographs do not show soft tissues particularly well, but indirect evidence seen on plain films often indicates rotator cuff injury. These may include spurring on the undersurface of the acromion or AC joint, cystic changes in the greater tuberosity, calcifications within the rotator cuff, and possibly a high-riding humeral head. The most definitive imaging technique to help with the diagnosis of rotator cuff injuries is magnetic resonance imaging (MRI). A well-done MRI with a high field magnet is typically excellent at determining the presence or absence of tendinosis, partial tearing or full-thickness tearing, and also provides specific information as to the size and location of the injury. It also provides information as to chronicity and reparability of the tear by revealing the extent of atrophy or fatty infiltration of the various rotator cuff muscles.
MRI – normal Rotator Cuff
MRI – Rotator Cuff tear
I have been diagnosed with a rotator cuff tear. Do I need surgery?
Not necessarily. Many studies have documented that a high proportion of the population over 60 years of age have asymptomatic or minimally symptomatic rotator cuff tears. Therefore, it is very possible that your painful rotator cuff condition, especially if insidious in onset, will respond favorably to conservative measures and not require any surgical intervention. Standard and often very successful treatments may include rest from offending activities, judicious use of anti-inflammatory medications, cortisone shots, and physical therapy. Physical therapy typically involves a supervised and home exercise program designed to selectively balance and strengthen the four muscles that comprise the rotator cuff. With gentle performance of these exercises several times a day on an ongoing basis, many patients will obtain relief of their symptoms and their strength will return. Exercises do not allow the torn rotator cuff to "heal" but can allow the remaining intact cuff to take over the function of the injured portion. In those who continue to have symptoms despite conservative treatment, surgical repair of the rotator cuff is the most effective way to eliminate pain and restore strength.
One situation is in which prolonged conservative management may not be particularly effective and in which surgery is recommended is a large tear due to a discrete traumatic incident. Studies have shown that the chances for a good surgical result are markedly improved if there is not a substantial delay in treatment, i.e., beyond a few months.
What actually is done when a surgeon repairs a torn rotator cuff?
First, the rotator cuff is identified and frayed or degenerated tissue is debrided (trimmed) back to healthy tissue. This healthy edge of tissue is then brought back to its normal site of insertion on the upper arm. This must be done without excessive tension and may involve different mobilization techniques to do so. The tendon edge is then secured back in place with strong sutures placed through tunnels created in the bone or alternatively attached to suture anchors that are securely embedded into bone.

Rotator cuff tear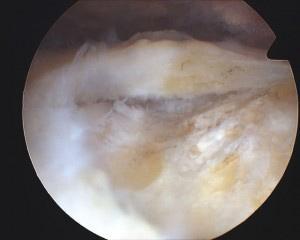
Tear debrided
Anchor placed in bone
Sutures placed in tendon
Rotator cuff repaired
The rotator cuff repair can be done through a standard open incision, a "mini-open" incision or arthroscopically. A standard open approach is historically the classic way to repair the rotator cuff. It requires a three- to four-inch incision anteriorly through which the deltoid muscle is detached from the acromion, so as to allow access to the underlying cuff. For the "usual" rotator cuff tear, this is typically a reliable, effective way to perform rotator cuff repair.
A "mini-open" repair may use a similar sized skin incision, but instead of detaching the deltoid, this muscle is split in line with its fibers for a short distance. Spreading the muscle fibers apart with a retractor and rotating the arm one way or another allows access to the underlying cuff. Because a large tear is difficult to repair through this mini-open incision, this approach is most frequently used when the preoperative evaluation clearly shows a small tear in the supraspinatus and there is no suggestion of other problems in the shoulder.
Many surgeons will routinely begin a rotator cuff repair by scoping the shoulder to confirm the size and location of the tear and to diagnose and treat other intra-articular abnormalities. Small tears can then be repaired through this "mini-incision."
Arthroscopic rotator cuff repair: Arthroscopy is a minimally invasive technique in which the surgical site is accessed through multiple small "poke hole" incisions and visualized with the use of an arthroscope, a long, tube-like instrument with lenses, fiber optics and attached camera. Similar-sized (1/4" X 8") surgical instruments are used to perform the operative work. This is in contrast to a standard open procedure in which the surgery is done through one larger incision in the front of the shoulder typically three to four inches in length. Fundamentally, the goals of surgery and the end result are usually the same, but simply stated, different paths are taken to get there.
What are the differences between an arthroscopic approach versus an open approach?
With the open approach, once the skin incision has been made, the deltoid muscle has to be detached anteriorly from the acromion bone to gain access to the underlying rotator cuff. Through this anterior incision the entire torn rotator cuff must be accessed. For small- or medium-sized tears, rotation of the arm can bring the torn tendon into view quite well usually, but with large or massive tears, it can be difficult, if not impossible, to see and operate on all the torn structures, especially those that are far posterior or medial. With the arthroscopic technique, which utilizes typically four or five poke hole incisions (portals) spaced around the shoulder from posterior to anterior, it becomes much easier to visualize and access the far posterior and medial aspects of the shoulder and rotator cuff. For this reason, large and massive tears can oftentimes more successfully be repaired arthroscopically. In addition, the arthroscopic portals do not require detachment of the deltoid; instead the muscle fibers are spread apart slightly rather than being cut. This fact eliminates the potential problem of a failed deltoid re-attachment which, although uncommon, can be disabling. For these reasons, it is accurate to say "several small incisions do not add up to one large incision."
Are there advantages to the arthroscopic approach to rotator cuff repair?
Yes, definitely, the main one being the ability to visualize and treat other pathological conditions inside the shoulder joint which are known to frequently co-exist with rotator cuff tears, i.e., DJD, loose bodies, labral tears and biceps lesions. With the open approach, even a large tear will allow visualization of only a small portion of the inside of the joint, whereas arthroscopically the entire inside of the joint can be assessed.
One category of problems very frequently associated with rotator cuff tear is biceps lesions, including tendonitis, tearing or instability. Loose bodies or cartilaginous debris are commonly seen with osteoarthritis and labral tears. All of these can be difficult to visualize with plain x-rays and even MRI is
not 100% accurate. Arthroscopy offers the most comprehensive way to thoroughly evaluate the shoulder and thereby increase the likelihood of a successful result that might otherwise be compromised by a missed diagnosis.
Does a rotator cuff repair heal faster if done arthroscopically?
No, the repaired tissues require the same amount of protection and time to heal regardless of which technique is used. A patient may often feel better sooner with an arthroscopic surgery versus an open surgery simply because there has been less surgical dissection of the surrounding muscles. Because of this improved comfort, a disciplined approach to carefully protecting the repair the first several weeks after surgery is necessary to maximize the likelihood of a successful result.
Will the surgery require a hospital stay? What about pain control after surgery?
Occasionally a patient will require an overnight stay in the hospital for either pain control or management of medical issues, but the great majority of these rotator cuff repairs are done as an outpatient. Prior to surgery, the anesthesiologist may provide an interscalene block or the surgeon may perform a suprascapular nerve block, both of which can provide for significant postoperative pain relief. In addition, the actual incision sites can be "numbed" with local anesthetic, which lasts for up to several hours after surgery. Finally, prescriptions for narcotic pain medication can be provided to help with pain management the first several days post-surgery.
How long does it take to recover from a rotator cuff repair?
The purpose of the sutures used in rotator cuff repair is to temporarily hold the tendon in proper position securely until healing takes place. No active use of the shoulder muscles is allowed for the first six weeks. To this end, the arm is placed in a sling/immobilizer and is typically taken out frequently only for passive range of motion exercises. At approximately six weeks, enough healing has taken place where active motion is instituted, as well as passive stretching. Formal supervised physical therapy is usually begun at this time to aid in the restoration of motion and strength. Ultimately, the patient is transitioned to a home exercise program. Continued improvement, comfort and function usually take place over a four- to six-month period and even longer with large or massive tears. In most cases patients can safely return to moderate recreational and work activities at four to six months after surgery and sooner for lighter activities.
The physicians and staff at Longview Orthopedic Associates are available to help you with your painful shoulder. Please feel free to call us at 360-501-3400 to schedule an appointment.
4 Mentions of “Rotator Cuff Tears”
- Dr. Blackstone Attends Arthroscopy Conference
November 24th, 2009 at 7:33 am - Dr. Blackstone Attends Arthroscopy Conference
November 24th, 2009 at 7:38 am - Blackstone Touts PIC-NOIA Connection
November 25th, 2009 at 7:43 am - Toni Stisser
July 23rd, 2010 at 11:06 pm