
About carpal tunnel syndrome
Carpal tunnel syndrome develops when a large nerve – the median nerve – is compressed inside your wrist. This nerve controls feeling in your thumb, index finger and thumb side of the ring finger. The median nerve also controls the muscles at the base of your thumb. The condition gets its name from the eight carpal bones that surround the median nerve in your wrist, forming a tunnel to your hand.
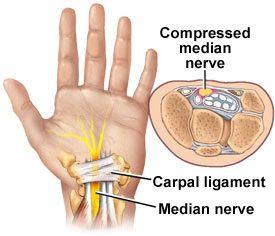
Carpal tunnel surgery releases pressure on median nerve.
The tunnel is just big enough for the median nerve and several tendons to run through it. Anything that makes the tunnel smaller (such as arthritis) or makes the tendons larger (such as thickening of the tendon linings) can cut off the circulation to the nerve. When this happens, you notice pain, numbness and tingling in your fingers.
Causes of carpal tunnel syndrome
Pressure on the median nerve can be caused by
- A wrist injury or a fracture of the wrist or the end of the forearm
- Frequent use of vibrating hand tools
- Any repetitive, forceful motion with the wrist bent, especially when done for prolonged periods without rest
- Rheumatoid arthritis
- Osteoarthritis
- Hypothyroidism and, less often, hyperthyroidism
- Diabetes
- Pregnancy
- Amyloidosis
- Acromegaly
- Systemic lupus erythematosus
Carpal tunnel syndrome can also be caused by underlying medical conditions including
Symptoms of carpal tunnel syndrome usually improve or go away when these underlying medical conditions are treated – or in the case of pregnancy, after the baby is born.
In many cases, the syndrome has no specific cause – in spite of the widespread belief that everyone in the work force is at risk. Jobs that require you to grip something repeatedly and forcefully or hold your fingers or wrists in an abnormal position may contribute to the condition in some people, but studies seeking to find a cause-and-effect relationship are inconclusive.
One clear finding from these studies is that frequent computer use doesn’t cause carpal tunnel syndrome, though it may worsen your symptoms. Several studies have found no relationship between computer use of up to seven hours a day and risk of carpal tunnel syndrome.
What increases your risk?
- Being female and middle-aged. Women are three times as likely as men to develop carpal tunnel syndrome. Doctors aren’t sure why. Fluid retention caused by hormone shifts may be a factor, as may having large breasts. So might the fact that women’s carpal tunnels are smaller than men’s.
- Obesity. Obesity increases your risk of carpal tunnel syndrome. Numerous studies have found more than twice as many carpal tunnel syndrome cases among the obese as among those with average weights.
- Genetics. Your genetic makeup may increase your risk of carpal tunnel syndrome. Researchers have found that in fraternal twins, the chance that both twins will develop carpal tunnel syndrome is significantly lower than that in identical twins, who share all the same genes. One specific – but rare – hereditary nerve disorder seems to cause carpal tunnel syndrome in a small number of people.
- Smoking. People who smoke cigarettes may experience worse symptoms and slower recovery from carpal tunnel syndrome than nonsmokers do.
How common is carpal tunnel syndrome?
Carpal tunnel syndrome affects about three out of every 100 people in the United States, although some estimates place the number higher. It is one of the most common causes of partial disability – both temporary and permanent. Slightly more than half of those who miss work because of carpal tunnel syndrome miss 31 days in one year. Up to 50 percent of people who have carpal tunnel syndrome have it in both hands.
Left untreated, carpal tunnel syndrome can lead to irreversible nerve and muscle damage. Fortunately, permanent nerve damage usually can be avoided if you’re diagnosed and treated early. Among people with a clear diagnosis of carpal tunnel syndrome, treatment relieves most of the pain, tingling and numbness. On the other hand, many people treated for carpal tunnel syndrome report persistent problems, and a few say their hands never get back to normal.
Symptoms of carpal tunnel syndrome
Carpal tunnel syndrome usually develops gradually. Pressure on the median nerve produces a specific pattern of numbness, tingling and pain that usually is worse at night. As the condition worsens, you may lose some hand strength and dexterity. You may experience any or all of these symptoms
- Numbness, burning, tingling or pain in the hand or fingers – but not in the little finger
- Increased discomfort at night or first thing in the morning
- Increased discomfort with prolonged grasping or flexing of the wrist
- Temporary symptom relief when you "shake out" your hands
- Hand weakness, especially loss of pinch strength or difficulty holding and picking up objects
- Loss of feeling in your thumb, index and middle fingers, and the thumb side of your ring finger
- Shrinkage or weakness of the muscle at the base of your thumb
- Inability to distinguish temperature changes
Diagnosing carpal tunnel syndrome
No single test can tell for sure if you have carpal tunnel syndrome. Instead, your doctor reviews your medical history and does a physical exam, then may arrange for you to have one or more tests.
During a physical exam for suspected carpal tunnel syndrome, your doctor examines your hands, arms, shoulders and neck. Your doctor may also
- Show you a hand diagram and ask you to mark those places where you experience numbness and tingling. One clue that it might be carpal tunnel syndrome is if you don’t have symptoms in your little finger. That’s because the median nerve doesn’t provide sensation to it. Hand diagrams are one of the most helpful diagnostic tools doctors use.
- Examine muscles at the base of your thumb for signs of shrinking (atrophy).
- Check to see how sensitive to touch your index finger is compared with your little finger.
- Check your ability to feel vibrations or mildly painful sensations on your fingers. Diminished ability to feel these sensations (hyperalgesia) may suggest that you have carpal tunnel syndrome.
Common diagnostic tests
During your exam, your doctor may give you the following tests to help diagnose carpal tunnel syndrome:
Phalen’s test.In this test, you place your elbows on the table with arms up. Bend your wrists down as far as you can while pressing the backs of your hands together for 30 to 60 seconds. If you feel tingling or numbness, it may mean that you have carpal tunnel syndrome.
Tinel’s test.Your doctor taps on the median nerve at your wrist. If you feel tingling or a shock-like sensation in the fingers served by the median nerve, you may have carpal tunnel syndrome.
Compression test.For this test, your doctor will apply constant pressure to the median nerve for 30 seconds. If you feel tingling or numbness, you may have carpal tunnel syndrome.
Additional tests
None of the tests above is completely accurate, possibly leading to an incorrect diagnosis – positive or negative. A physical exam doesn’t always provide the answer either. That’s why your doctor may order these additional tests
X-rays.These helps rule out arthritis, bone spurs, fractures, tumors, cysts and gout.
Nerve tests.These tests help measure how well your median nerve is working. Nerve tests are the most reliable tests for confirming if you have carpal tunnel syndrome. Two types of nerve studies are routinely used to diagnose carpal tunnel syndrome.
- Electromyograms (EMGs).EMGs measure the tiny electrical discharges produced in muscles. A thin-needle electrode is inserted into the muscle or muscles your doctor wants to examine. An instrument records the electrical activity in your muscle at rest and as you contract the muscle. The test can help determine if you have nerve damage in your hand caused by long-term pressure on the median nerve.
- Nerve conduction studies.These are the most sensitive tests for confirming if you have carpal tunnel syndrome. They measure the speed at which electrical impulses travel along your nerves. Electrodes are taped to your fingers and arm. A mild shock passes from one electrode to the other through your median nerve. If the electrical impulses slowdown in the carpal tunnel, this is the strongest evidence that you have carpal tunnel syndrome.
Diagnostic ultrasound
Ultrasound is a new and alternative way to help determine if you have carpal tunnel syndrome. Its use for this purpose is still being studied and may not be available in your area. Sound waves are bounced off your hand and wrist to create images of nerves, muscles and tendons. Carpal tunnel syndrome can make the median nerve look thinner than normal. Ultrasound can’t test nerve function, though, so it can only suggest a diagnosis.
Treatment options
All traditional treatments for carpal tunnel syndrome attempt to relieve pressure on the median nerve as it passes through the carpal tunnel in your wrist. Which treatment choice you make depends on the following
- How severe your symptoms are
- What’s causing your symptoms
- How long you’ve had them
Treatments for carpal tunnel syndrome fall into two general categories: surgical and nonsurgical. Both have potential risks and benefits.
Nonsurgical
Nonsurgical treatments include a sequence of options, starting with simple steps you can take, such as activity modification, and moving on to more involved treatments, such as splints and corticosteroid injections.
Most people with carpal tunnel syndrome should at least give nonsurgical treatments a try. These treatments work best if you haven’t lost any hand strength. They might work – saving you the cost of surgery and the discomfort and time away from work that follows surgery. If they don’t work, you’ll know in a few weeks, and you can then have surgery.
Activity modification
Wrist position is key to controlling your carpal tunnel syndrome symptoms. The carpal tunnel is most narrow when your wrist is either bent down or cocked back all the way. It is largest when the wrist is straight. For this reason, changing how you do repetitive hand activities or avoiding those activities altogether can help. The more your wrist is bent, the more pressure is put on your median nerve. To protect your hands, take these precautions
- Take breaks.When doing activities that require repetitive, forceful motion with your wrists bent, stop every 15 to 20 minutes and gently stretch and bend your hands and fingers. When working with vibrating equipment, wear gel-padded gloves. These absorb vibration that can cause swelling around the median nerve. If possible, change activities for several minutes every hour.
- Most important, rethink what you’re doing. Often, it’s possible to do the same task and avoid extreme wrist positions, simply by changing your position or that of the object you’re working on. Or, you can modify the grip or handle of your tools, for example, going from a straight handle to a pistol grip.
- Relax your grip.Avoid gripping too hard when driving, writing or using hand tools. Most people use more force than necessary when doing hand tasks. When working on a computer, for example, tap the keys softly. When writing, use a thick pen with an oversized, soft grip adapter and free-flowing ink. That way you won’t have to grip the pen tightly or press as hard on the paper.
- Use proper posture.Poor posture causes your shoulders to roll forward, shortening your neck and shoulder muscles and compressing nerves in your neck. This can affect your wrists, fingers and hands because some nerves in the upper body eventually connect to the median nerve. When compressed, they affect how they send signals to and from your hand.
- Reduce wrist bending.Avoid bending your wrist all the way up or down. A relaxed middle position is best. Keep your computer keyboard at elbow height or slightly lower. A keyboard wrist pad placed in front of the keyboard further relieves wrist strain. However, resting with too much pressure on the wrist pad or on a hard surface may exacerbate symptoms.
- Keep your hands warm.Pain and stiffness are more likely to occur if your hands are cold. Adjust the room temperature or wear fingerless gloves.
Splinting
Splints (braces) are the most commonly used nonsurgical treatment for carpal tunnel syndrome. Splints that immobilize the wrist in a neutral (unbent) position are most likely to relieve discomfort. An unbent wrist maximizes the size of the carpal tunnel, which reduces pressure on the median nerve, relieving your symptoms.
You can buy ready-made splints at a medical-supplies store. Or you can ask your doctor to have custom-made splints made for you. Both are equally effective, although many people find custom-made splints more comfortable to wear. In either case, you may find splints make certain hand movements difficult to do.
You may need to wear a splint for a few days to a week or more before noticing significant improvement. Some studies show that continuous splinting – wearing a splint both day and night – is more effective than wearing it just at night. Others, however, show little or no added benefit from 24-hour splinting, particularly in terms of symptom relief. Also, many people find that a splint restricts their hand and wrist movements too much to be worthwhile at work and around the house, so night wear alone is a good option.
Splints are safe, relatively inexpensive and give many people with carpal tunnel syndrome excellent short-term relief from their symptoms. Besides relieving discomfort, splints can sometimes improve conduction of nerve impulses along the median nerve, which can improve strength, dexterity and sensation.
Splints are most likely to work for you if you’ve had mild to moderate carpal tunnel syndrome symptoms for one year or less. Splints may be a good choice if pregnancy is causing temporary discomfort you can’t tolerate.
Physical therapy and exercise
Sometimes, physical therapy or special hand exercises relieve mild to moderate symptoms of carpal tunnel syndrome.
Gliding exercises
Some people who don’t get adequate relief from splints and activity modification do get more relief when these treatments are combined with nerve and tendon gliding exercises. Gliding exercises alone may help, but usually not as much as when they’re combined with other treatments.
- Tendon gliding exercises.You move your fingers through five positions with your wrist in a neutral (unbent) position.
- Median nerve gliding exercises.You move your hand through six positions while your wrist is in a neutral position.
During both types of gliding exercises, you maintain each position for seven seconds. Repeat each set of exercises five times, three to five times each day.
Gliding exercises relieve pressure on the median nerve. During the exercises, your median nerve is exposed to a higher pressure, followed by a lower pressure. The pressure changes are believed to shift the point on the median nerve that’s under the most pressure as it passes through the carpal tunnel. The exercises may also loosen and stretch the carpal ligaments, further easing pressure. Gliding exercises may also encourage movement of blood out of the carpal tunnel, further relieving fluid pressure on the nerve. Similarly, the exercises may help reduce water retention in the carpal tunnel.
Contrast baths
These baths can help reduce carpal tunnel swelling. To do this therapy, soak your hand in warm water for five to 10 minutes, then in cold water for one minute, then back and forth between hot and cold. You typically do this twice each day. Contrast baths are often done in combination with gliding exercises to relieve symptoms.
Ultrasound
Directing ultrasound waves at the carpal tunnel can be helpful in mild to moderate carpal tunnel syndrome, though results have been mixed. In one study, 20 sessions of therapy during seven weeks significantly relieved discomfort and improved hand function after two weeks, seven weeks and six months. Other studies have shown no benefit.
Exercises and physical therapy don’t change the natural course of carpal tunnel syndrome, which tends to worsen over time. These treatments are typically most effective in temporarily relieving symptoms of mild to moderate carpal tunnel syndrome. Keep in mind, though, if you change how you do routine activities and treat any underlying medical condition that might be worsening your carpal tunnel syndrome, you may notice permanent improvement.
Drug therapy
Drug treatment of carpal tunnel syndrome attempts to reduce any inflammation in the carpal tunnel that might put pressure on the median nerve. These medications are commonly used
NSAIDs. If tendinitis or another inflammatory condition accompanies your carpal tunnel syndrome, you can relieve some of the pain by taking nonsteroidal anti-inflammatory drugs (NSAIDs). These drugs include ibuprofen (Advil, Motrin, others), naproxen sodium (Anaprox, Aleve, others) and aspirin – either prescription or over-the-counter.
NSAIDs are unlikely to relieve your symptoms if inflammation isn’t causing your discomfort – and most people don’t have inflammation around their nerve. NSAIDs do nothing to relieve other carpal tunnel syndrome signs and symptoms, such as tingling, numbness or hand weakness. Even when an inflammatory condition is present, NSAIDs may be most effective when used in combination with splinting, activity modification and gliding exercises. When used in such combination, it’s difficult to know if the NSAIDs are adding to the known benefit of those other treatments. Even nonprescription NSAIDs may cause side effects in some people if taken for a long time. Consult your doctor before taking NSAIDs.
Diuretics.Diuretics are high blood pressure medications sometimes prescribed on the theory that fluid retention in the carpal tunnel can cause pressure on the median nerve. There’s no evidence this is true. Diuretics have undesirable side effects and are rarely used.
Corticosteroids.If you don’t get adequate relief from splints or activity modification, your doctor may inject your carpal tunnel with a corticosteroid, such as cortisone. Corticosteroid injections can be quite effective in providing temporary relief from carpal tunnel syndrome symptoms. The main effect of these drugs is to reduce inflammation, whether it’s from arthritis, asthma or some other condition. Because surgery for carpal tunnel syndrome rarely reveals any evidence of inflammation, though, the reasons for corticosteroids’ effectiveness in carpal tunnel syndrome are unknown. Corticosteroid pills don’t work as well as corticosteroid injections.
Corticosteroid injections will most likely give you long-term relief from carpal tunnel syndrome symptoms if you
- Have mild to moderate symptoms for one year or less
- Have no loss of feeling or strength in your hand
Corticosteroid injections may provide significant short-term relief from pain, tingling and numbness. Often, some relief is immediate. Relief then builds over time, often peaking about one month after injection. The length of time an injection is effective varies greatly from several weeks to more than a year. Relief may last longer if your carpal tunnel syndrome symptoms are mild to moderate at the time of injection.
You may get renewed relief from a second injection. However, some trials have found that fewer than half of those who got good relief from the first injection got adequate relief from the second.
Complications with corticosteroid injections are rare. However, the risk of complications increases as you have more injections. These rare complications include nerve injury and tendon rupture.
Pros and cons
For most people with carpal tunnel syndrome, doctors try nonsurgical treatments before opting for surgery. However, the decision is a personal one influenced by the cause and severity of your symptoms and your feelings about surgery. When deciding whether to try nonsurgical options or skip them, keep these points in mind